
Charlotte Houston and Milwaukee Prehospital EMS Research Node Center (CHaMP)
Charlotte, Houston, and Milwaukee Prehospital (CHaMP) is a node of PECARN composed of three diverse EMS agencies that collectively respond to nearly 350,000 EMS calls per year including 25,000 pediatric calls. Our Mission is to conduct innovative and relevant collaborative pediatric prehospital research.
The three CHaMP EMS affiliates are dedicated to providing high-quality prehospital care and believe that research is an important aspect of providing high-quality care. Each agency has previously participated in successful prehospital randomized clinical trials and has cultivated a culture that values research. Together, the CHaMP investigators and EMS agencies aim to find the answers to important questions that will improve the health of children who access the emergency response system.
The CHaMP Investigators are also dedicated to increasing the scope, quality, and quantity of pediatric EMS research. Therefore, CHaMP is developing online research education as well as promoting opportunities and science through our Facebook page.
This project is supported by the Health Resources and Services Administration (HRSA), Maternal and Child Health Bureau (MCHB), Emergency Medical Services for Children (EMSC) Targeted Issues grant program, Grant No. H34MC26201 for $900,000. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government.
CHaMP's Emergency Medical Services Affiliates:
- Milwaukee County EMS, Milwaukee, WI
- Mecklenburg EMS Agency (Medic), Charlotte, NC
- Houston Fire Department EMS, Houston, TX
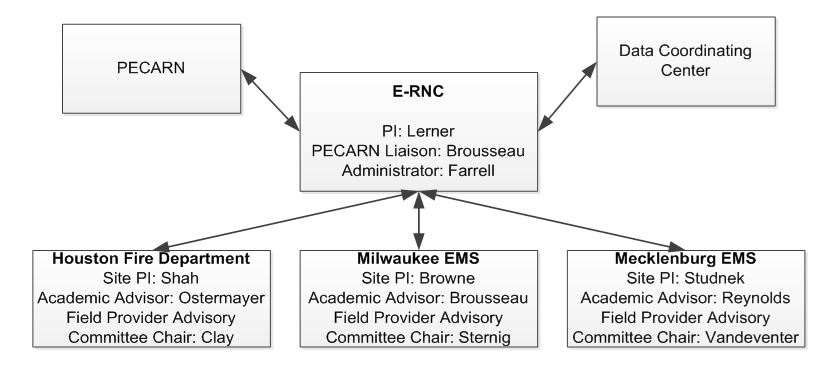
The EMS Research Node Center (E-RNC) is CHaMP’s administrative hub and is housed at the Medical College of Wisconsin. The Houston Fire Department, Milwaukee EMS, and Mecklenburg EMS are CHaMP’s three EMS Affiliates. Each EMS affiliate has a site Principal Investigator who oversees the site's involvement in CHaMP. There is also an Academic Advisor at each site who will support the site's Principal Investigator who will conduct pediatric prehospital-based research.
Mecklenburg EMS (Medic)
Mecklenburg EMS (Medic) is a leader in clinical outcomes in the prehospital setting and provides a unique opportunity to conduct outcomes based research from initial patient contact to final hospital disposition. Medic is a municipal agency overseen by a Board of Commissioners comprised of representatives from both local healthcare systems and the County. Medic is an all Advanced Life Support level EMS agency with at least one paramedic responding on all ambulances dispatched to a medical emergency. Medic is dispatched to all medical emergencies within the County using a priority dispatch system to triage calls for severity. On a majority of medical calls first responders are simultaneously dispatched with first response provided by the city fire department or one of 19 county first response agencies. First response units are typically made up of between two and four Emergency Medical Technician-Basic trained automated external defibrillator equipped personnel responding on a fire engine or rescue unit. All medical providers within the EMS system follow the same protocols and provide care under the same medical director. Protocols at the Basic Life Support level form the base of all care protocols with only Medic paramedics permitted to perform care at the Advance Life Support level. Online and offline medical direction is provided by the EMS medical director and assistant medical director, or any emergency physician at a local receiving hospital. Protocol development, education, and clinical oversight are directed by the agency’s Quality Management Committee which is a sub-committee of the agency’s Medical Control Board. The Medical Control Board is comprised of local physicians with experience in emergency medicine, EMS, trauma, surgery, cardiovascular disease, and orthopedics. These physicians hold a variety of local, state, and national EMS leadership roles.
Medic emergently treats over 87,000 people per year, 15% of which are under the age of 21. Medic transports patients to nine affiliated paramedic-receiving hospitals which are operated by the two healthcare systems within the county. Both healthcare systems participate in the Medic Research Committee which receives its direction from the Quality Management Committee and is comprised of physician and non-physician researchers interested in outcomes based prehospital research. Medic has a Medical Services Division which is comprised of six full-time educators, who are all paramedics and former field training officers who provide essential training and educational support for any out-of-hospital clinical research protocols. Medic also contracts with the Center for Prehospital Medicine at Carolinas Medical Center to supplement education as needed. The quality improvement department at Medic consists of six individuals who provide data analysis support for ongoing research initiatives and conduct initial review and development of potential research projects. Engaged physicians from the agency medical control board, consistent medical direction, and a robust quality management system support the high quality out-of-hospital care that is provided in the county and also ensures consistent implementation of out-of-hospital clinical trials.
Medic uses an electronic patient care reporting and data collection system. Medic works closely with both healthcare systems in the county which includes the academic institution, Carolinas Medical Center. The EMS Medical Director for the County has an academic appointment at Carolinas Medical Center, works clinically in the emergency department, and has a strong track record of supporting and guiding EMS research. Medic has partnered with the Carolinas Medical Center and Novant Healthcare to conduct numerous research projects.
Houston Fire Department
The City of Houston’s EMS system is composed of a single Fire Department. The Houston Fire Department provides a two-tiered EMS system made up of over 3,500 providers, all of which are trained as firefighters and have at least Basic Life Support (BLS) training with an EMT-Basic certification. Nearly 15% of the firefighters are trained to provide Advanced Life Support with paramedic certification. Oversight of daily operations lies with the Assistant Fire Chief over EMS. All 911 calls for the City are directed to a single Public Safety Answering Point, the Houston Emergency Center, where civilian dispatchers and prehospital providers utilize computer aided dispatch protocols to triage calls, deliver care, and dispatch personnel. Prehospital providers follow agency-wide protocols to triage, evaluate, manage, and transport patients to over 40 area hospitals that include two level-one trauma centers and one free-standing tertiary pediatric hospital. Online and offline medical direction, protocol development, education and clinical oversight are provided by three full-time board certified emergency medicine physicians, all of whom are EMS fellowship-trained, and one part-time board certified pediatric emergency medicine physician. The Medical Director and Pediatric Medical Director both serve on local, state, and national EMS policy-making bodies including the Texas Governors EMS and Trauma Advisory Council and the National EMS Advisory Council. The State of Texas is one of 47 States that require that every paramedic pass the National Registry EMT Certification exam before practicing patient care.
The Houston Fire Department responds to over 220,000 calls per year resulting in approximately 170,000 transports. Approximately 14% of their patients are children. Forty percent of pediatric calls originate in the home, and 44% are injury related. The Houston Fire Department has a rich history of participating in research, including a 1985 study which was arguably one of the first major prehospital studies and identified a lack of benefit from anti-shock trousers. Since 1985 they have continued to conduct research including participating in randomized clinical trials evaluating a blood substitute for the treatment of trauma and a mechanical chest compression device for the treatment of out-of hospital cardiac arrest.
Milwaukee County EMS
The Milwaukee County EMS system provides a robust and established clinical laboratory, experienced in successfully completing numerous NIH-funded translational research protocols. The Milwaukee County EMS system is fire department based and provides Advanced Life Support (ALS) level services. It provides a tiered response with first response units composed of at least two Emergency Medical Technician-Basic trained, automated external defibrillator equipped personnel from either a privately owned ambulance or a municipal fire engine. Simultaneously, ALS ambulances are dispatched with the first response units. ALS ambulances are staffed by at least two paramedic level responders employed by one of the 12 municipal fire departments that service the region. All paramedics within the EMS system follow the same protocols and provide care under the same Medical Director. Online and offline medical direction, protocol development, education and clinical oversight are provided by a team of six board certified emergency medicine physicians. These physicians hold a variety of local, state, and national EMS leadership roles including serving as Wisconsin’s State Medical Director and Immediate Past President of the National Association of EMS Physicians.
The EMS system emergently treats over 40,000 people per year, 10% of which are under the age of 21 years. Milwaukee County EMS transports patients to 15 affiliated paramedic-receiving hospitals which participate in the Milwaukee Emergency Medicine Research Consortium, an experienced and proven research association that provides continued research interventions, monitoring, follow-up, and/or hospital medical record review for patients entered in out-of-hospital trials. Five, full-time educators, who are both paramedics and registered nurses, provide essential training and educational support for any out-of-hospital clinical research protocols. Physician online medical control and a well-tested quality management system support the high quality out-of-hospital care that is provided in the county and also ensure consistent implementation of out-of-hospital clinical trials. Although the system is made up of 12 distinct fire departments, each agency’s prehospital care providers participate in research as if they are from one agency. All 12 agencies allow a local research committee, composed of representatives from the various local stakeholders (including the public), to determine if a proposed research project should be implemented in the community.
Contact CHaMP
(414) 955-1117 | (414) 805-6464 (fax)