
Collaborative for Healthcare Harm, Hazard, and Risk Reduction and Prevention (CHiRP)

Mission
Core Principles:
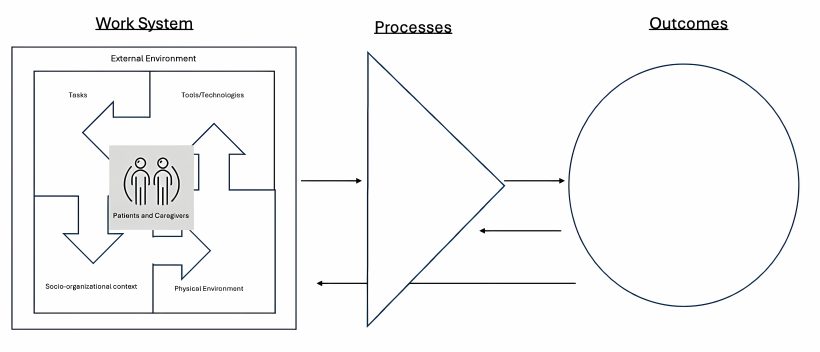
- Healthcare harm is the result of hazards and poor design within complex sociotechnical systems- involving people, environments, tools and technology-and their interactions with other system components.
- Healthcare providers are a source of safety through their adaptative actions.
- The phenomena labeled as “error” is a product of complex system interactions and NOT the cause of harm events. Instead, error is a symptom of poorly designed systems. Importantly, the same systems that yield good outcomes also lead to harm to patients and healthcare workers.
- Harm reduction and prevention require collaboration with non-healthcare disciplines including (but not limited to) human factors engineers, psychologists, experts in design, patients and families, and clinicians.
- That said, zero harm can be an aspiration but never a goal. It is literally impossible to achieve zero harm because the system is complex and dynamic.
Who Should Join?
How to Join
Publications, Presentations, Mentorship, and Consultations
Two Accepted or Published Manuscripts
• Ladell M, Jacobson N, Yale S, McDermott K, Papautsky E, Catchpole K, Scanlon M. The problem with how we view medical (and diagnostic) error in emergency medicine. Academic Emergency Medicine. 2025 March; 00:1-8. PMID: 40033164.
• Ladell M, Jacobson N, Yale S, Venkitachalam R, McCarthy C, Suenkens K, Catchpole K, Nimmer M, Scanlon M, Papautsky E. Getting SSPOT to Run: Development of a Novel Direct Observational Tool for Usage in Clinical Settings. Applied Ergonomics
One International Presentation
• SEIPS Model Scottish Quality and Safety Fellowship
Three International Posters (all with MCW students as first authors)
• Scheduled Medication Administration in a Pediatric Intensive Care Unit: It’s Harder Than You Think
• Workflow Disruptions and Adaptive Nursing Strategies in Pediatric Intensive Care Medication Administration
• Data Acquisition in the Emergency Room, It’s Harder Than You Think!
Two National Presentations
• Systems Engineering Initiative for Patient Safety Introduction. Solutions for Patient Safety PETT Scan Project
• PETT Scan Introduction. Solutions for Patient Safety PETT Scan Project
Nine Regional Presentations
• Four at Wisconsin Chapter of the American College of Emergency Physicians; Two presented by MCW students
• One at the National Association of EMS Physicians
• One at the Midwest PICU Collaborative
• One at Purdue University
• Two at Washington University
Numerous Local Presentations
• MCW Neurology Grand Rounds
• MCW Pediatric Grand Rounds
• MCW Medicine Quality Committee
• Multiple presentations to the Quality Improvement and Patient Safety Scholarly Concentration
• Two presentations to the Health Systems Management Professionals Scholarly Concentration
• Two presentations to the Good Doctors Thread
• Multiple presentations to the MCWAH QI and Safety Elective
• Two educational sessions on Systems Thinking using the game, Friday Night in the ER
Mentorship and Advisors
• At least 30 MCW medical and graduate students
• One Emergency Medicine resident, three Pediatric Critical Care Fellow, and one Pediatric Hospital Medicine Fellow
Consultations
• Pediatric Readiness in Community ED Settings
• Milwaukee County EMS Safety Review Tool
• Event Review and PETT Scan Use for PHM (multi-disciplinary with Neurosurgery and nursing)
• Incorporation of PETT scan into post-simulation debriefing for Sports Medicine Interdisciplinary Simulation (Yale, McDermott)