
Medical College of Wisconsin Stroke, Neurointervention, and Critical Care
Meet Our Stroke Neurointervention & Critical Care Team

Hatim Attar, MD
Interim Division Chief, Neurology at Zablocki VA Medical Center; Associate Professor
Specialty: Inpatient Stroke



Marek Cierny, MD
Assistant Professor
Specialty: Inpatient Stroke



Joshua E. Medow, MD, MSc, PhD, FAANS, FACS, FNCS, FAHA, FCCM, FAMIA
Division Chief, Inpatient Neurology; Professor
Specialty: Adult Neuro ICU


Adam C. Wadina, MD
Assistant Professor
Specialty: Vascular Neurology/Stroke (Ambulatory & Inpatient)
Department Info
Selected Disorders and Conditions
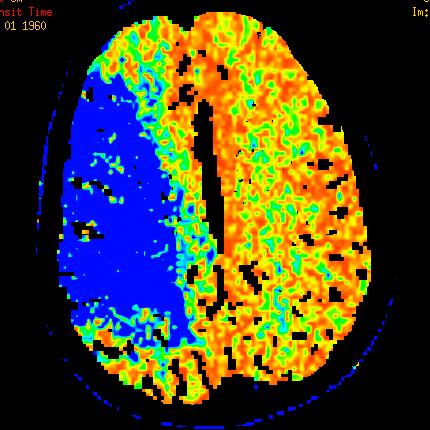
Acute stroke affects nearly 800,000 Americans annually making it the leading cause of disability and the 4th leading cause of death in the United States. About 80% of these strokes are due to a blockage of a blood vessel known as an “ischemic stroke.” This leads to inadequate blood flow to a part of the brain and causes a focal neurological deficit such as speech difficulty, numbness or weakness of an arm or leg, or vision loss. Timely restoration of blood flow to the brain is critical to prevent permanent damage to the affected brain tissue.
Time is brain, which is why rapid decisions are needed in the treatment of acute ischemic stroke. Patients experiencing an acute stroke require expedited diagnostic imaging of the brain and swift evaluation and management. Those who present within 4.5 hours from symptom onset and meeting specific criteria are eligible for a “clot busting” medication known as tissue plasminogen activator (tPA) administered through an IV. Patients who are not eligible for the IV medication may benefit from endovascular therapy using local administration of a medication at the clot in the blood vessel or clot removal with a device.
Knowing the signs and symptoms of stroke is important. A way to remember the stroke signs is F.A.S.T.:
- Face: Ask the person to smile to determine if one side of the face droops.
- Arms: Ask the person to raise both arms to determine if one drifts down.
- Speech: Ask the person to repeat a simple phrase to determine if speech is clear or not.
- Time: Call 911 immediately with any of these signs.
Act F.A.S.T. and call 911 immediately.

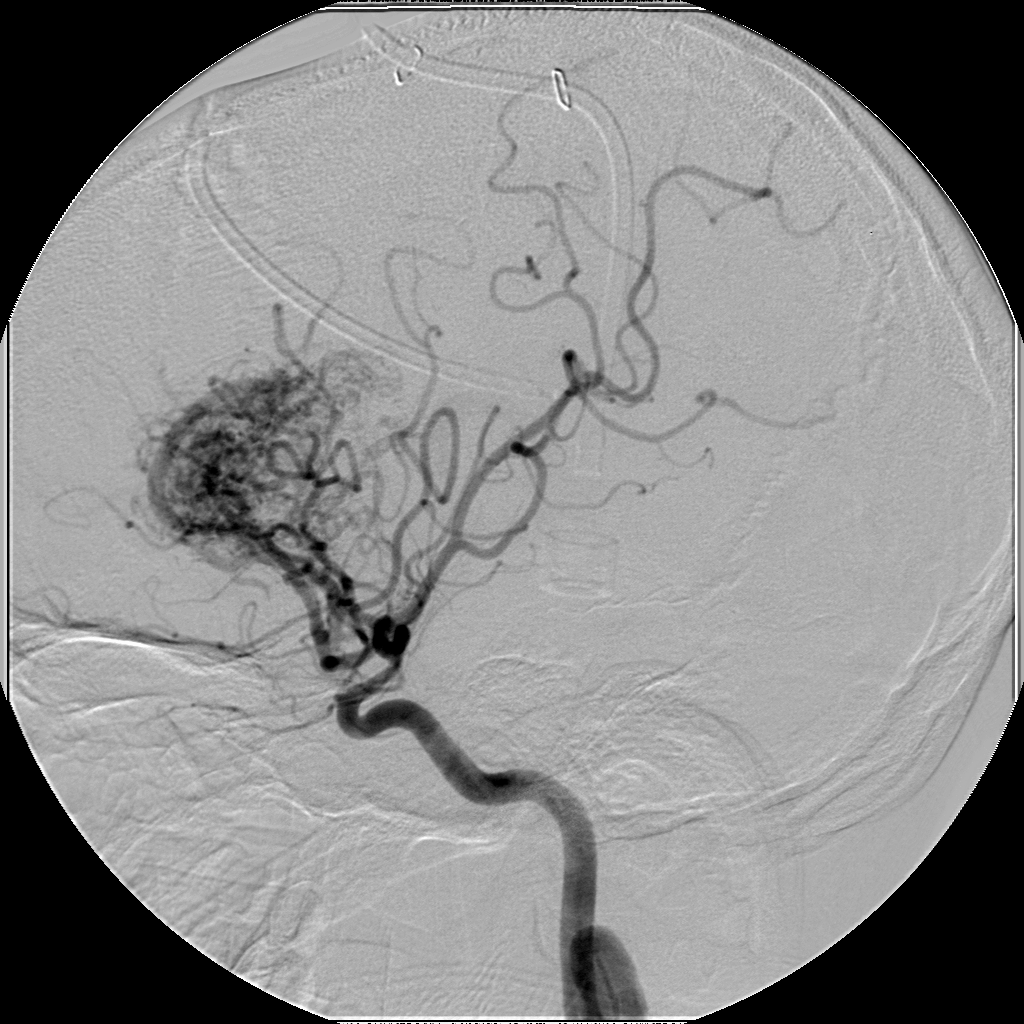
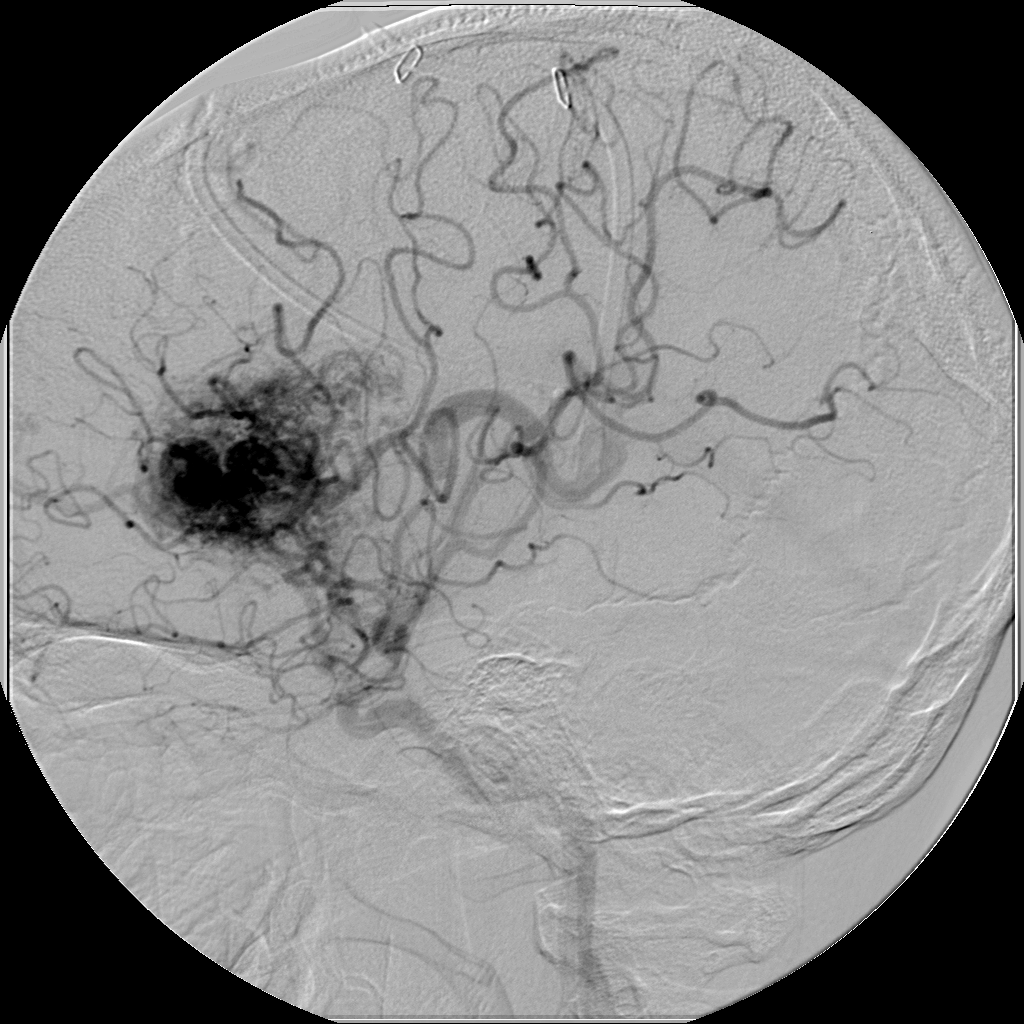
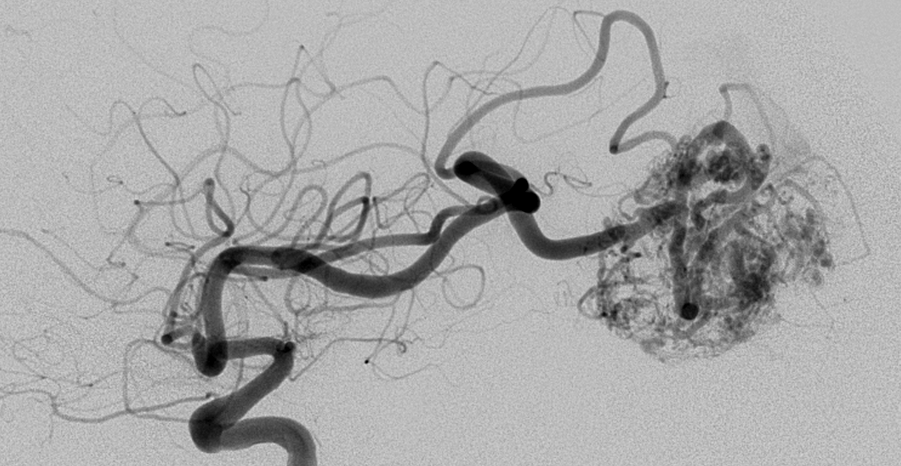
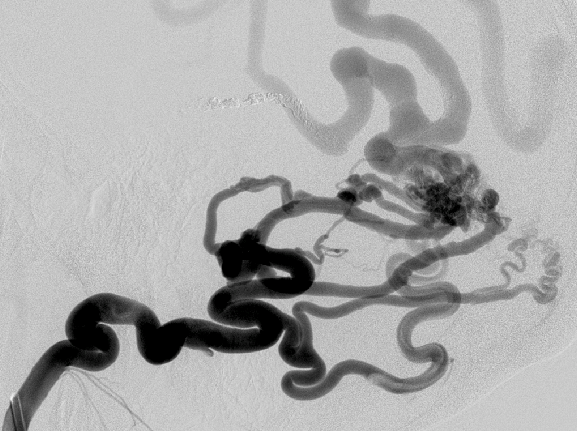
An arteriovenous malformation (AVM) is an abnormality of the blood vessels that may be present in the brain or spine and is believed to develop at the time of embryonic development. The malformation results in shunting of blood from arteries to veins, bypassing capillary blood vessels that serve normal brain tissue. The condition is rare and is thought to be present in about 0.1% to 0.2% of the population. The blood vessel abnormalities may not cause any significant neurologic problems and be discovered incidentally, or they may cause a wide variety of symptoms depending on the location. An AVM may be identified after headaches, a seizure, or rupture that causes bleeding. The workup for a patient with a suspected AVM often involves imaging studies such as CT or MRI of the brain, as well as catheter cerebral angiography to comprehensively define the abnormality. Various management strategies are then considered including observation, endovascular embolization, surgical resection, and gamma knife radiation.
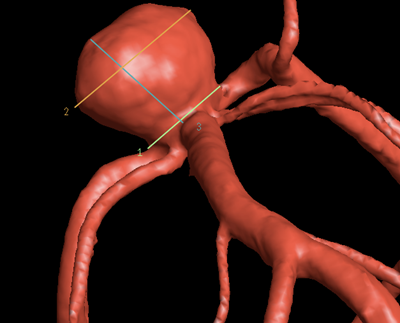
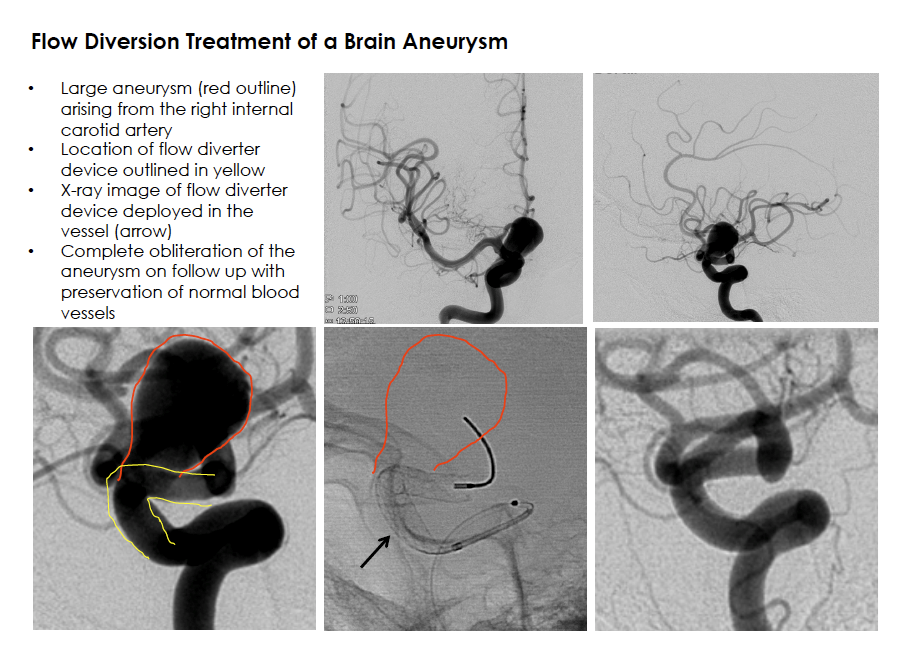
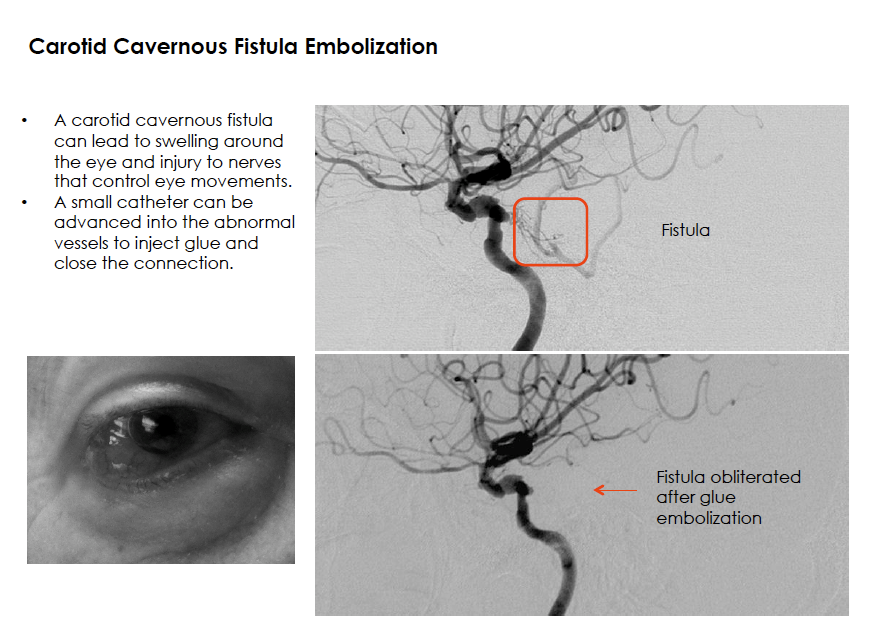
A brain aneurysm (cerebral aneurysm) is a bulge arising from the side of an artery wall in the head. It may be present from birth or develop after injury to the blood vessel. It has been estimated that up to about 5% of the population has a cerebral aneurysm. Symptoms of an aneurysm can include headaches or focal neurological deficits (such as a cranial nerve injury leading to difficulty with eye movement). Although rupture of an aneurysm is uncommon, the bleeding into the space surrounding the brain known as subarachnoid hemorrhage causes a severe headache and carries a high risk of severe neurologic injury and death. Risk factors for cerebral aneurysm growth include a family history, smoking, high blood pressure, and certain medical problems including polycystic kidney disease. Unruptured aneurysm treatment varies depending on several factors including the aneurysm shape, location, and a patient’s overall health. Management strategies include observation, endovascular coil embolization or blood flow diversion, and microsurgical clipping. A ruptured cerebral aneurysm is an emergency that requires urgent treatment.


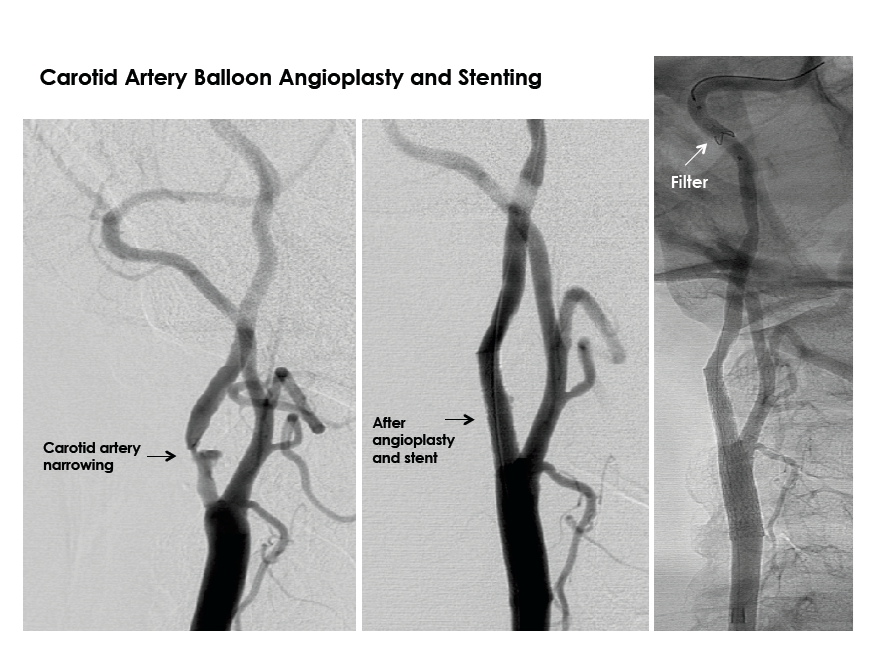
The carotid arteries are two large blood vessels in the neck that supply oxygenated blood to the brain. Carotid artery disease includes atherosclerosis which leads narrowing of the artery due to buildup of fatty substances and cholesterol deposits known as plaque. Stenosis, or narrowing, of these arteries can lead to stroke, a leading cause of death and disability in the United States. Signs and symptoms of carotid artery disease include transient ischemic attacks (TIA) or stroke. Patients may report changes in vision, strength, sensation, speech or other abnormalities. Evaluation of the carotid arteries can be performed with several non-invasive imaging methods including ultrasound, MRI, and CT. Management depends on various factors including the degree of narrowing, symptoms, and overall health. Treatment can include a combination of medicines to combat progression of plaque formation, lifestyle modifications, open surgery, or minimally invasive endovascular treatment.


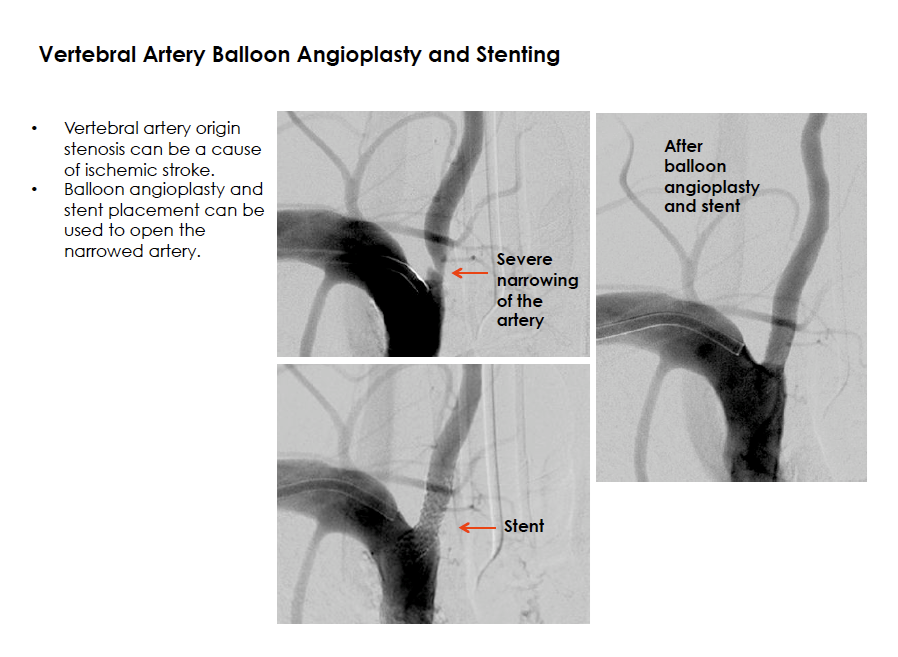
The vertebral arteries are a set of paired arteries that supply oxygenated blood to the back part of the brain. Atherosclerosis, or hardening of the arteries due to fatty substance deposition and plaque buildup, can lead to narrowing of the blood vessels. Patients may present with stroke or transient ischemic attack (TIA) symptoms such as a focal deficit of vision loss, dizziness, speech difficulty, or numbness or weakness of an arm or leg. Evaluation of the vertebral arteries can be performed with non-invasive imaging such as an MRI or CT scan. Patients with this condition can benefit from lifestyle changes and a medication regimen that will limit the progression of the narrowing. For patients who experience further narrowing and symptoms despite medications, some may benefit from an endovascular procedure to open the blocked artery.

Selected Procedures
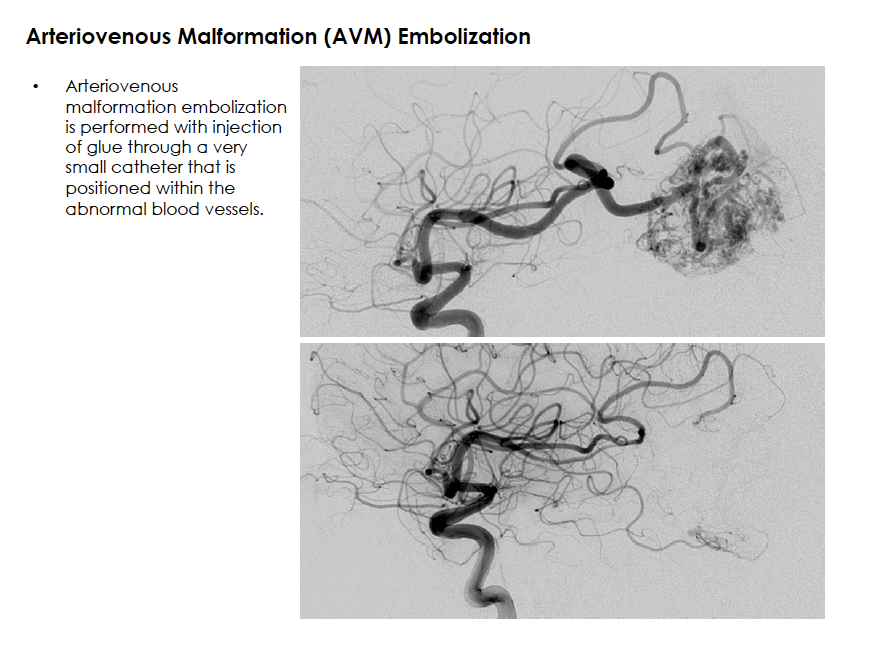
Embolization of brain and spine arteriovenous malformations (AVMs) and arteriovenous fistulas (AVFs)
An arteriovenous malformation or dural arteriovenous fistula is an abnormality of the blood vessels that causes shunting of blood from an artery to a vein, bypassing normal tissue. This high-flow system may pose a risk for bleeding. Many characteristics of the abnormality may be important in deciding the best management approach. Endovascular embolization therapy is a method of injecting a “liquid embolic” or glue-like material into the target vessel to stop blood flow through the abnormality. A microcatheter (a very small hollow plastic tube) is carefully navigated to the abnormal connection between the artery and the vein. A glue material is then injected through the catheter to fill the abnormal collection of blood vessels, effectively closing the communication. The catheter is removed and the solidified glue remains within the blood vessels to permanently close the abnormality. This procedure may be performed alone or in conjunction with other treatments including open surgical resection or radiosurgery therapy.
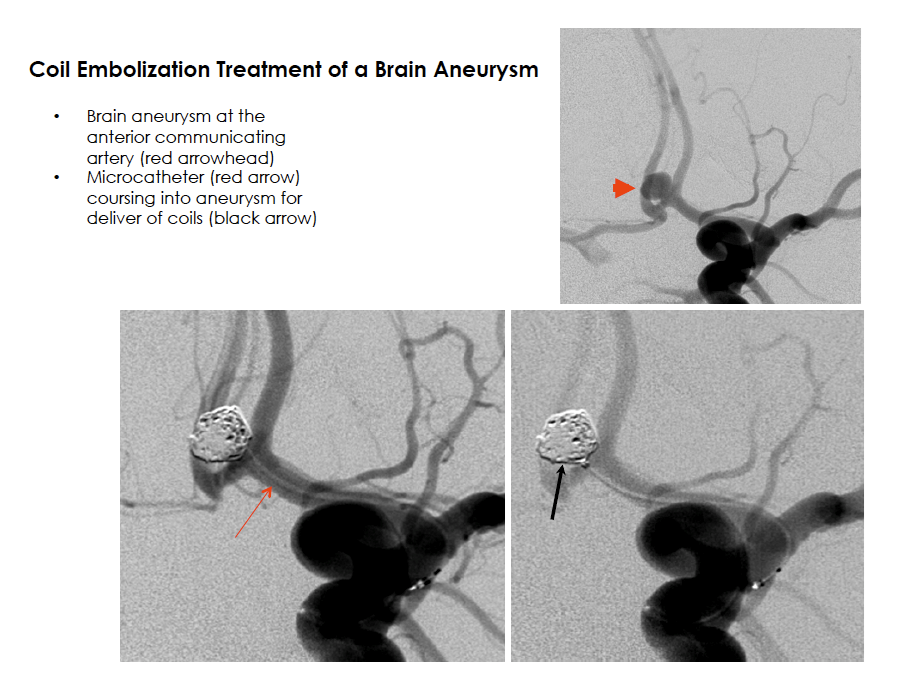
Some brain aneurysms can be closely observed with periodic surveillance imaging. For aneurysms that require treatment, endovascular therapy can be performed from inside the blood vessel. Access to the inside of the aneurysm is achieved with the same techniques used in diagnostic catheter cerebral angiography, by advancing a catheter (a hollow plastic tube) through an artery in the leg and navigating it to the blood vessels in the brain. After the catheter is positioned at the site of the brain aneurysm, several techniques are used to close the aneurysm and prevent any further blood flow entry. Coil embolization, or “coiling,” is the most commonly practiced endovascular treatment for brain aneurysms. In this procedure, a very small catheter is advanced into the aneurysm and platinum coils are sequentially introduced to create a tightly packed coil mass within the aneurysm, thereby promoting clot formation within the aneurysm, and preventing entry of blood flow. In some cases, a stent or balloon is required to remodel the neck of the aneurysm for safe coil placement and to promote healing. A balloon is temporarily inflated at the aneurysm neck, while a stent is permanently implanted to provide continuous support at the opening of the aneurysm. Newer technology and techniques now include flow diversion devices for endovascular aneurysm treatment. In this method, a mesh stent-like device is placed within the vessel and across the neck of the aneurysm to divert blood flow away from the aneurysm and down the normal course of the blood vessel. This promotes aneurysm closure and scaffolding for healing of the blood vessel wall. The rapid pace of technology development and evolution of techniques for endovascular repair of brain aneurysms will likely continue to advance safety and efficacy of minimally invasive therapies.
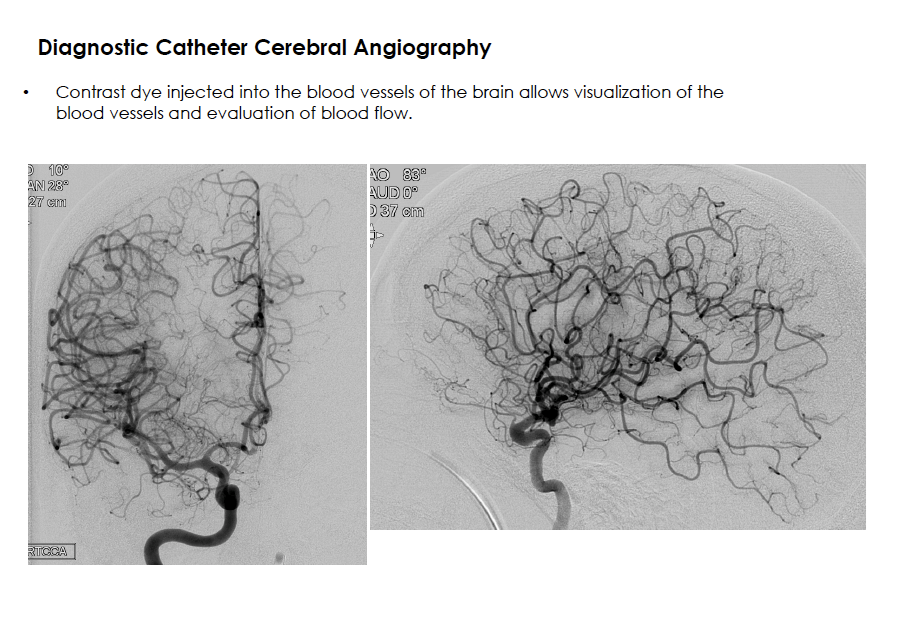
The procedure is commonly performed with the patient awake but very sleepy, under “conscious sedation.” Sedation medications are administered to achieve patient comfort. During contrast injections, a patient may experience a sensation of warmth, flashes of lights, intermittent dizziness, or unusual tastes. These symptoms are well-tolerated, brief, and pass within seconds.
At the completion of the procedure, the catheter and sheath are removed, and pressure is applied to the leg or a small plug is placed to close the artery access site. The patient then recovers with flat bed rest for approximately 3 to 6 hours before returning home the same day.
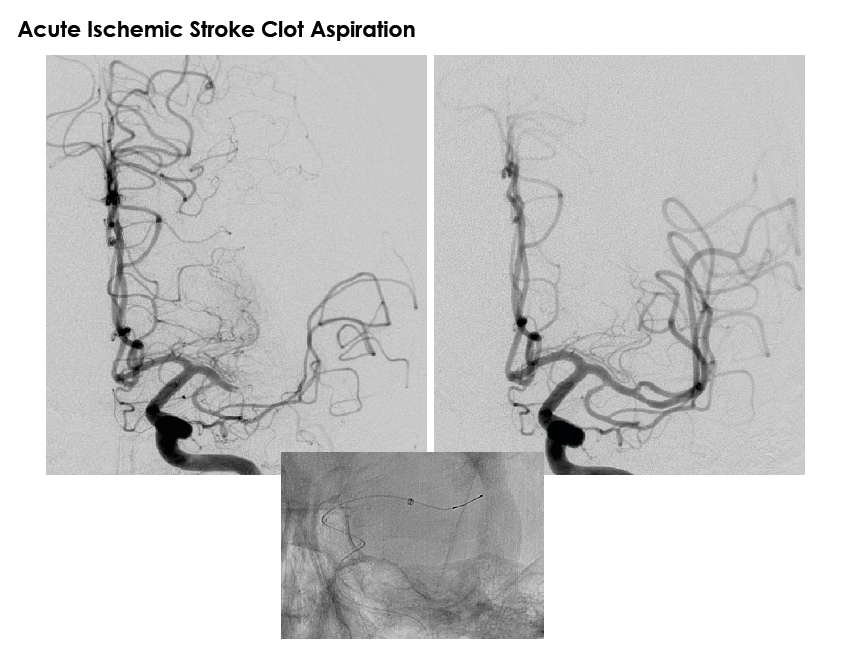
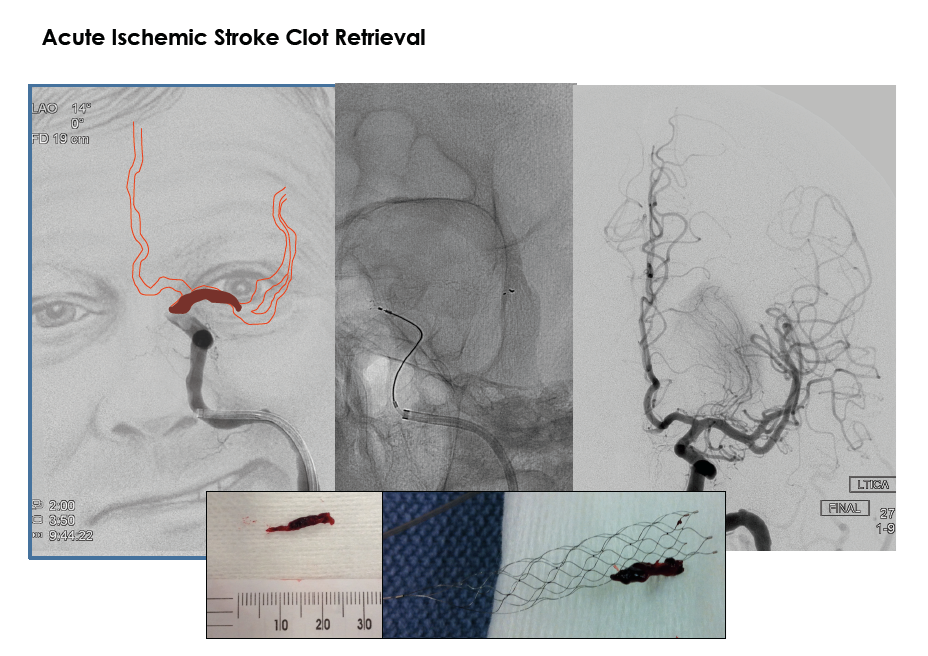
The impact of ischemic stroke upon healthcare in the United States is staggering. Extensive research has attempted to unlock methods of safely restoring blood flow to the brain and protect patients from progression to permanent brain damage. In 1996, the United States Food and Drug Administration approved the use of intravenous tissue plasminogen activator (IV tPA) for use in the treatment of acute ischemic stroke in selected patients. This “clot-busting” medicine has been shown to improve patient outcomes when it is administered within the first few hours of a stroke. Among those patients who are not candidates for an intravenous medication, some may benefit from an endovascular method of removing a blood clot. Endovascular methods include navigating a small catheter (a hollow plastic tube) through the blood vessels to the location of the blockage and using one of several therapies. After a catheter is positioned within the blocked artery, tPA can be injected to dissolve the clot, or a device can be used to suction the clot (aspiration) or trap the clot and remove it from the body. Time is brain, which is why methods of opening a blocked artery are performed in the first few hours of an ischemic stroke.
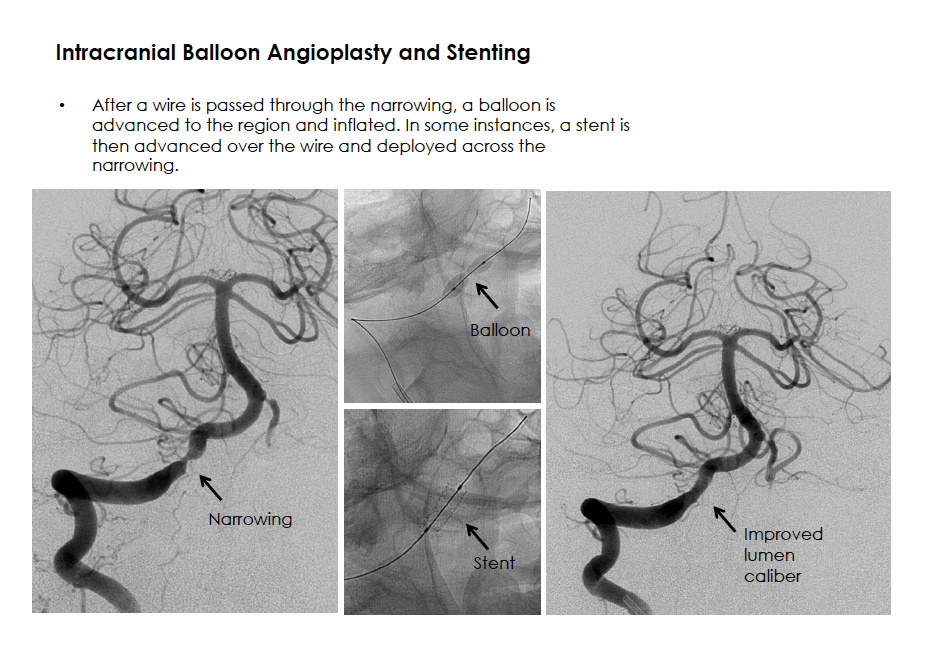
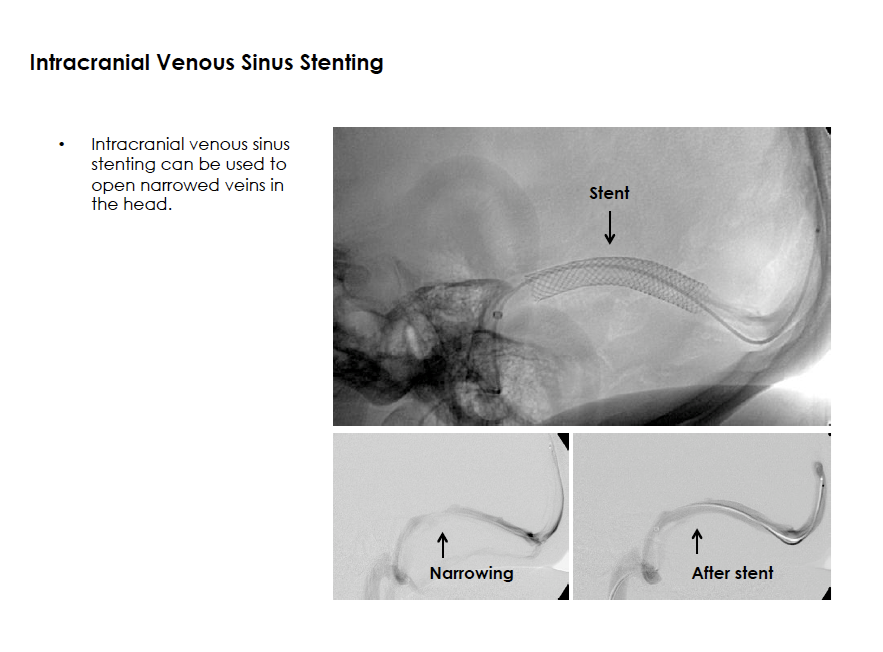
Intracranial venous sinus abnormalities can obstruct the outflow of blood from the head. In some patients who have chronically elevated intracranial pressures, venous outflow obstruction may be a related finding. For evaluation, patients often undergo diagnostic brain imaging such as MRI or MR angiography, detailed eye examination, and an endovascular procedure to perform manometry testing to evaluate intracranial pressures in several locations. Selected patients may benefit from placement of a stent within a dural sinus of the head to improve venous outflow. The stent is delivered using standard neuroendovascular techniques and on occasion a balloon is also inflated within the stent to ensure optimal placement.
Disclaimer
The information on the Division of Stroke, Neurointervention and Critical Care website is for educational purposes only and is not intended as medical advice. While general information regarding the conditions treated and procedures performed is posted, this information is not a substitute for professional medical advice, diagnosis, or treatment. All patients are treated with individualized care based on independent professional judgment and experience in each specific case.