
Case Study 25: 16-year-old non-verbal male with history of retinopathy of prematurity
Original Authors: Gao Zangzee Yang, Aparna Ramasubramanian, MD, Heather Stiff, MD
HPI
A 16-year-old non-verbal male with a history of retinopathy of prematurity (ROP) (born at 24 weeks, 1 lb 1 oz) presented to the clinic with a 2-week history of a red left eye as reported by his mother. The patient indicated irritation by rolling his eyes around. His mother reported that he often squints and winces when exposed to light. No other ocular concerns reported.
Past Ocular History
Retinopathy of prematurity (stage 4A), bilateral optic atrophy, exotropia.
Ocular Medications
None
Past Medical History
Prematurity 24 weeks (1 lb 1 oz)
Cerebral Palsy
Microcephaly
Global developmental delays
Cystic encephalomalacia
Periventricular leukomalacia
Ventriculomegaly
Wheelchair bound
H/o grade 4 intraventricular hemorrhage
H/o necrotizing enterocolitis with intestinal resection
Seizure disorder
Presence of intrathecal baclofen pump
History of tracheostomy
Mild chronic lung disease of prematurity
Obstructive sleep apnea
Laryngomalacia
G-tube placement
GERD, S/P laparoscopic Nissen fundoplication
Chronic hepatitis
Neuromuscular scoliosis
Chronic pain disorder
Surgical History
S/P Panretinal Photocoagulation (PRP) both eyes (OU)
Past Family Ocular History
Non-contributory
Social History
Lives at home with parents and siblings
Attends school (10th grade)
Medications
Fluticasone
Ipratropium-albuterol
Linaclotide
Magnesium oxide
Melatonin
Montelukast
Ondansetron
Phenobarbital
Phytonadione
Rifaximin
Trazodone
Triamcinolone cream
Ursodiol
Acetaminophen
Albuterol
Baclofen
Bisacodyl
Calcium citrate
Zyrtec
Cholecalciferol
Clonidine
Diazepam
Esomeprazole
Famotidine
Allergies
No known drug allergies
ROS
Per HPI, otherwise negative
Ocular Exam
Visual Acuity (cc)
OD: Inconsistent blinks to light using an indirect ophthalmoscope at the brightest setting
OS: Inconsistent blinks to light using an indirect ophthalmoscope at the brightest setting
IOP (iCare tonometry)
OD: 15, 9 mmHg
OS: 51, 53, 41, 54 mmHg
Pupils
OD: 4.5 mm in dark; 3.5 mm in light; round, sluggish, no afferent pupillary defect (APD)
OS: 5.5 mm in dark; 5 mm in light; round, minimal reaction, no obvious APD
Extraocular Movements
OU: Roving eye movements with nystagmus. Ductions grossly full to volitional movements.
Confrontational Visual Fields (Toys)
Unable to test (UTT) due to delay
Slit Lamp:
| OD | OS | |
| External | Normal | Normal |
| Lids and Lashes | Normal | Normal |
| Conjunctiva/Sclera | White and quiet | Bulbar conjunctival injection |
| Cornea | Clear | Mild haze |
| Anterior Chamber | Deep and quiet | Deep |
| Iris | Round and sluggish | Round and minimally reactive |
| Lens | Clear | Clear |
| Anterior Vitreous | Normal | Normal |
Dilated Fundus Examination:
| OD | OS | |
| Disc | Pallor/atrophy | Pallor/atrophy |
| Macula | Normal | Normal |
| Vessels | Prominent vascular attenuation, notable temporally | Prominent vascular attenuation, notable temporally |
| Periphery | PRP scars nasally and temporally | Brief view of PRP temporally |
Imaging/additional tests:
RETCAM Fundus Photography – image of right eye followed by left eye
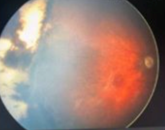
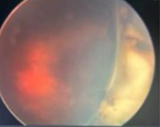
RETCAM fundus photos of the left eye reveal mild haze of the vitreous, complete pallor of the optic nerve, mottled macula, attenuated vessels, and 360 laser with temporal peripheral vitreoretinal traction with retinal elevation, but no retinal detachment.
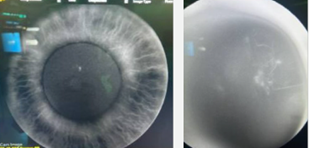
RETCAM


RETCAM photos of the anterior segment shows normal appearing anterior segment of the right eye and perilimbal injection of the left eye.
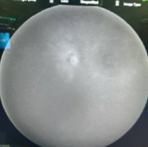
Ultrasound (B-scan)
The B-scan ultrasound of the left eye showed temporal retinal elevation.
Ultrasound biomicroscopy (UBM)

Ultrasound biomicroscopy of the left eye reveals open angle with no obvious narrowing or closure.
Fluorescein angiography (FA) – all images of left eye
Fluorescein angiography of right eye shows no neovascularization of the retina or iris. Left eye showed iris neovascularization in the temporal pupillary border and showed temporal retinal neovascularization.
Medical College of Wisconsin Ophthalmology and Visual Sciences Case Studies
-
Ophthalmic Case Study 1
Acute right eye pain -
Ophthalmic Case Study 2
Red, itchy eyes -
Ophthalmic Case Study 3
Acute left eye pain and blurry vision -
Ophthalmic Case Study 4
Left eye pain and fuzzy vision 2 days after eye surgery -
Ophthalmic Case Study 5
Girl rubbing her R eye after trauma -
Ophthalmic Case Study 6
Red eye and pain on the left -
Ophthalmic Case Study 7
Vision loss L eye -
Ophthalmic Case Study 8
Crossed eyes -
Ophthalmic Case Study 9
White pupils -
Ophthalmic Case Study 10
Blurry vision in the left eye for 2 weeks -
Ophthalmic Case Study 11
Acute pain and burning in L eye -
Ophthalmic Case Study 12
Blurry vision in both eyes and headaches -
Ophthalmic Case Study 13
"Cannot see well" from left eye -
Ophthalmic Case Study 14
Blurry vision in both eyes -
Ophthalmic Case Study 15
Eye irritation and dryness -
Ophthalmic Case Study 16
2 brief episodes of vision loss in the R eye -
Ophthalmic Case Study 17
Routine eye exam -
Ophthalmic Case Study 18
8-year-old boy, difficulty seeing whiteboard -
Ophthalmic Case Study 19
8-year-old girl, wandering eye and double vision. -
Ophthalmic Case Study 20
Red eyelid lesion in an infant -
Ophthalmic Case Study 21
Female patient with optic nerve abnormality -
Ophthalmic Case Study 22
Left eye pain, tearing, redness, and photophobia -
Ophthalmic Case Study 23
1-year-old male presents with intermittent eye misalignment -
Ophthalmic Case Study 24
Left eye pain, redness, and blurry vision -
Ophthalmic Case Study 25
16-year-old non-verbal male with history of retinopathy -
Ophthalmic Case Study 26
69-year-old female presents for decreased visual acuity